Patient presented with one year of pain and restriction of terminal flexion. clinical ex. revealed stable knee with poorly localized pain on terminal flexion. No clear localising signs.. lachman1+ solid end pt. negative pivot shift. ocl and collateral stable. no clear meniscal signs except pain on terminal flexion
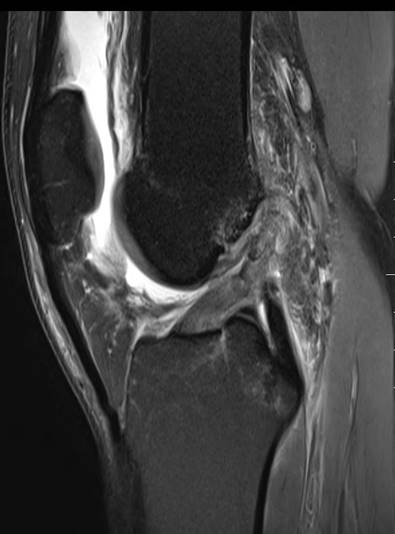
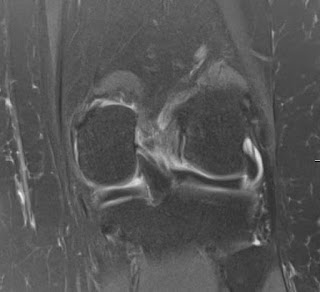
MRI shows celery stalk appearance with cyst posterior to ACL and between ACL and PCL.
treatment
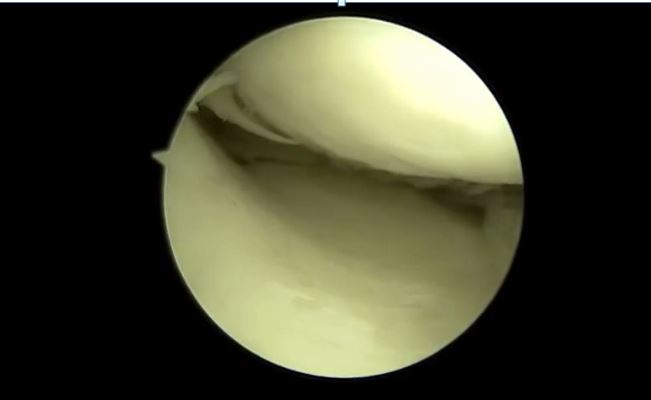
Arthro scopic cysyt decompression and intraligamentous microfracture inside the femoral attachment of ACL was done
t


6-week MRI shows a healing ACL with the absent cyst.
6 months postop

Is ACLshaving and reconstruction necessary or the trauma of multiple small shaver punctures to decompress and cause bleeding and microfracture to release MSCs into the ligament enough at least in some cases? The patient feels better and had full range of painless movement 1-month post-op