Supracondylar
femoral fracture is a devastating complication after a total knee replacement.
Supracondylar femoral fractures account
for about 0.3 to 2.5 %.. With rising numbers of knee replacements the
number of these fractures are going to rise. The treatment is technically challenging in type 2 fractures . In type 1 conservative treatment is acceptable and revision is advised in type 3
The benefits of
total knee replacement have been well documented. Periprosthetic fractures
involving distal femur, proximal tibia or patella especially during the
postoperative period causes considerable morbidity to the patient and is a
technical challenge to the treating surgeon.
Majority of these fractures occur after a trivial fall. Rheumatoid
patients receiving corticosteroid and immuno suppressant therapy, severe osteopenia and osteoporosis,
old people, women are at a greater risk for supra condylar fractures. Severe
osteoporosis makes fracture fixation difficult.
High incidence of supracondylar fractures (40-52%) has been reported
with anterior femoral notching.
Both
conservative and surgical modalities of treatment have been described in the
management of these fractures.
Favourable results have been documented in certain studies with conservative management . In general,
conservative methods may be utilized in type 1 fractures ( Lewis and Rorabeck ), provided the patients
are followed up with xrays at regular intervals . Displaced supracondylar
fractures (type 2) needs to be properly aligned and stabilized for an optimal
outcome. Stabilization using intramedullary nails, locking plates, external
fixators have been described. Type 3
fractures may require a revision with distal femoral replacement prosthesis or
a structural allograft.
Proper alignment
and stabilization of the fracture is mandatory for early mobilization of the
knee. In type 2 frequently the far
cortex is weak or communited, rigidity with a an intramedullary nail or a locking plate alone is suboptimal for
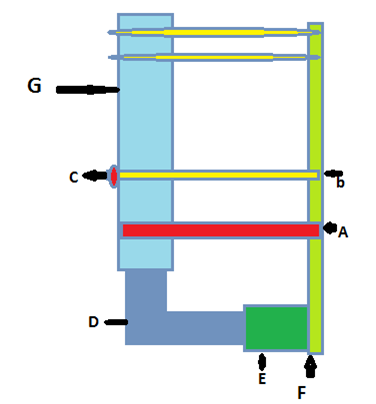
mobilisation. In such instances a
combination of a nail plate devise which
are interconnected and locked to each other (locked screw on the plate and a
locking nut on the screw and nail would increase the rigidity of the construct
enabling early mobilisation of the patient. A blue print for such a devise and introducing instrument is given below.
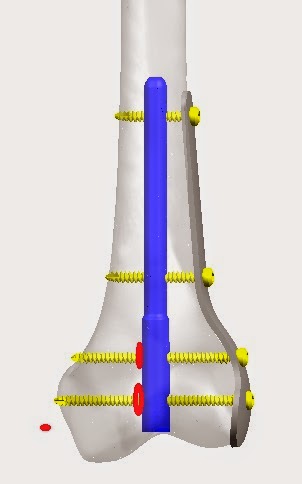
In 2009 following
difficulty in stabilising these distal femoral fractures, combination of a separate Intra medullary nail and a locking plate was used to stabilise and mobilise the elderly
above mentioned osteoporotic fracture.
This was repeated in bilateral case where in the nail was
removed to pass the distal locking
screws from the plate resulting in
translation of the distal fragment refer
pictures below. Both the fractures healed in 3 months
with no lag and loss of pre-fracture motion
Technique
Knee replacement
incision. A supracondylar nail 9 mm in diameter was passed through the distal
fragment and using this to reduce the
fragment and pass it retrograde into the proximal fragment. This avoids soft
tissue stripping and quick reduction of the fracture in anterior-posterior and
medial lateral planes with out soft
tissue stripping associated with reduction with a plate device. This nail
devise could be locked proximally and distally if possible or at this stage a
locking plate is passed through a MIPPO technique on the lateral femoral side through the same tkr incision and
locking screws can be applied distally though the incision and percutaneous
screws can be applied proximally. In the case
in picture on the right knee the nail was removed after the plate was
applied distally to facilitate screw
insertion resulting in translation in the medio-lateral plane. Therefore it was
decided to use both nail and plate in 3 further cases where in we obtained
stable reduction to facilitate immediate mobilisation.
With these results we attempted to design a
new implant ( nail plate device) to improve the technique and rigidity of fixation
jig to implant the nail plate devise
nail plate devise locking both together in cases of communition


 A waiting cultures including mycobacterium and fungal. All cultures were negative. Inspite of B tcp which was to reduce local infalmmmation by bringing in osteoblasts early. this happened. wouldn't peek implants be better as thet do not xause anty local reaction
A waiting cultures including mycobacterium and fungal. All cultures were negative. Inspite of B tcp which was to reduce local infalmmmation by bringing in osteoblasts early. this happened. wouldn't peek implants be better as thet do not xause anty local reaction