MSK imaging has improved leaps over the past 2 to 3 years. Use of 3 tesla magnets( minimum of 1.5 tesla). multichannel coils and joint specific coils for ankle. wrist and shoulder, specific sequences for cartilage have improved our diagnostic accuracy.
With insurance companies asking for MRI reports I feel it is mandatory that the imagologists update the skills and machinery to avoid leaving the poor patients troubled. I have many times seen patients refused insurance clearance for surgery with painful conditions which need surgical intervention due to incompetent reports and images. Oh yes, insurance and imaging companies are there for profit, but that should not affect the quality of care at the point of delivery.
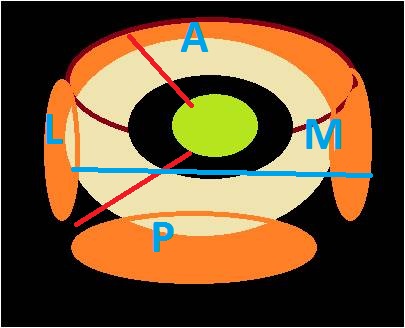
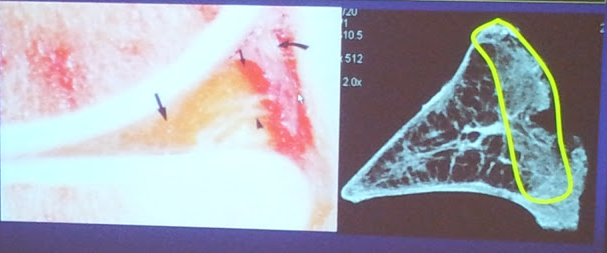
As for us orthopods and radiologists look at the quality of pics above even differentiating the red and white zones which could help plan repair or menisectomy more accurately. The radiologists should quantify,qualify and classify tears type 0 to 7 types( mesgarzadeh et al /1993.asses size and depth of cartilage lesions in addition to standard ligaments.
Specific cartilage sequences identify chondral injury in the presence of episodic pain despite "standard normal MRI reports" and asses healing using MOCART scores to be objective about results
I was pleasantly shocked to see some images from a 7 tesla machine.
I was pleasantly shocked to see some images from a 7 tesla machine.