Below are 3 cases send my fellow orthopods for comments. I have given my opinion and would appreciate and welcome other contributions for this interesting cases
Case 1- 47 year old lady with pain. Apparently patient refused an arthrodesis
 My views on case 1.
As she is 47 an arthrodesis is the first option in view of the complexity, one may not get the best bearings and position. if insistent, I would use possible a trabecular metal metaphyseal cone or sleeve with wedges to rebuild the lateral condyle. Tibia is standard wedge and stem. Patella would be major realignment problem. The BAJA could be corrected by using a smaller patellar button superiorly. We do not have the skyline view to comment
My views on case 1.
As she is 47 an arthrodesis is the first option in view of the complexity, one may not get the best bearings and position. if insistent, I would use possible a trabecular metal metaphyseal cone or sleeve with wedges to rebuild the lateral condyle. Tibia is standard wedge and stem. Patella would be major realignment problem. The BAJA could be corrected by using a smaller patellar button superiorly. We do not have the skyline view to comment
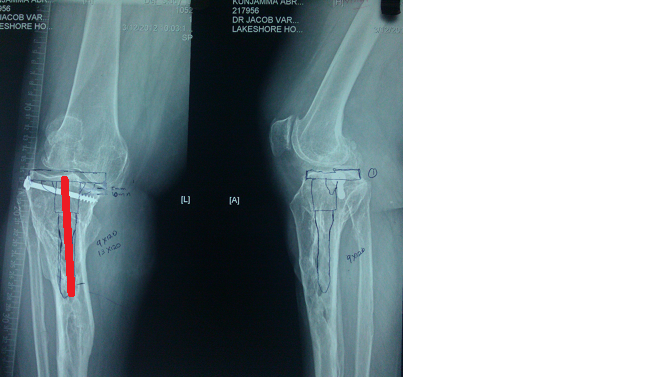
The answer to bonegrafting question would be if at all it should be an entire distal femoral allograft shaped with a conical proximal( Red Triangle) end jammed into the host metaphysis and protected with a by pass long stem( green line) as simple lateral condyle reconstruction alone is prone to resorption in the short to medium term. Even the method I described from elsewhere is prone to fractures and resorption in the medium term. You could argue that one wants to rebulit the bone.
I have one case where in I used the sculpted femoral head( no cartilage) from amrita bone bank to rebuild the lateral condyle in a trauma(bone loss) situation. after 6 months non wt bearing i did an arthroscopic arthrolysis and got 90 degree ROM. Tthinking about future TKR as the condyle appears vascurised on xray. No TKR as of yet as least to my knowledge.
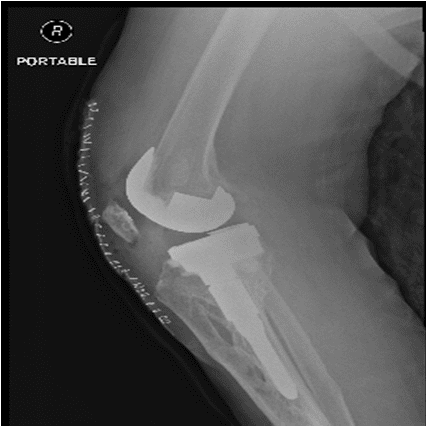
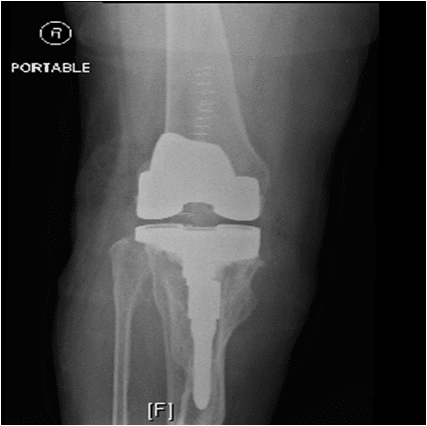
Below is vijays postop xray and comments ,
I used femoral metaphyseal cones and L wedges to build up the defect. Th Quadriceps was atrophic and patella was on the lateral gutter. Could mobilize by lateral release . Post op flexion is 80 now. Active extension is very weak.
Kindly opine
![]()
Of course we need better xrays to comment on alignment. He had a RHK back up incase. The metaphyseal cone gave him a stable paltform for the femur to build on.o
Case 2 .A case of 71 yr old female having bilateral FFD of 40 degrees
On the Lt knee in case 2 One needs to be careful of the MCL which, if incompetent would need a Rotating hinge back up. I feels if MCL is intact I would do try a primary knee or CCK with wedge and stem back up. Stems even if no wedges in view of the porosis and start PTH.
At 71 RHK is techinically less demanding.
I think the Rt side should be standard with just wedges and stem for tibia and a lateral femoral wedge at best. Watch out for intraop fractures and ligamentous avulsions
.Please send me the post op pics too if possible for all of us
Dr mahajan comments
On Right side - I will use medial tibial wedge & for lateral femoral condyle I will use distal & posterior wedge.I will need tibial as well as femoral stems.
The postop pics look fine. The rt femur is extended . It might be a stress riser if he falls. I would have stemmed the femur too. Consider PTH injections to build bone too
I